
Pluripotent Stem Cell Expansion And Scale-Up

Article inspired by a Tapas and TechTalks digital event. Fast Trak Centre for Advanced Therapeutic Cell Technologies (CATCT) team members shared insights from customer collaborations.
Building on a legacy of bioprocessing
Translating a long history of biopharma knowledge to cell therapies requires industrialization (i.e., standardizing biomanufacturing workflows and equipment to manage the complexities in making and delivering cellular therapies.) Production in mammalian cells has been dominated by monoclonal antibodies (mAb) and other proteins, where cells produce the protein of interest. Information about how these cells grow is widely available, because we're typically using intensely studied and well-established cell lines.
For cell therapies, however, the cells are the product. We're tapping into new cell sources with very different and unique characteristics. We do not have a lot of the historical data to fall back on, especially when it comes to scale-up. So, upstream process development (PD) is now a major area of focus.
Upstream PD is complex for stem cell therapies, because these therapies involve many manipulations during cell differentiation or even cell engineering. Decisions made early in research will impact the entire product life cycle, so it is important to consider a good process design early on.
Designing a modern process
Figure 1 shows a general workflow for PSC.
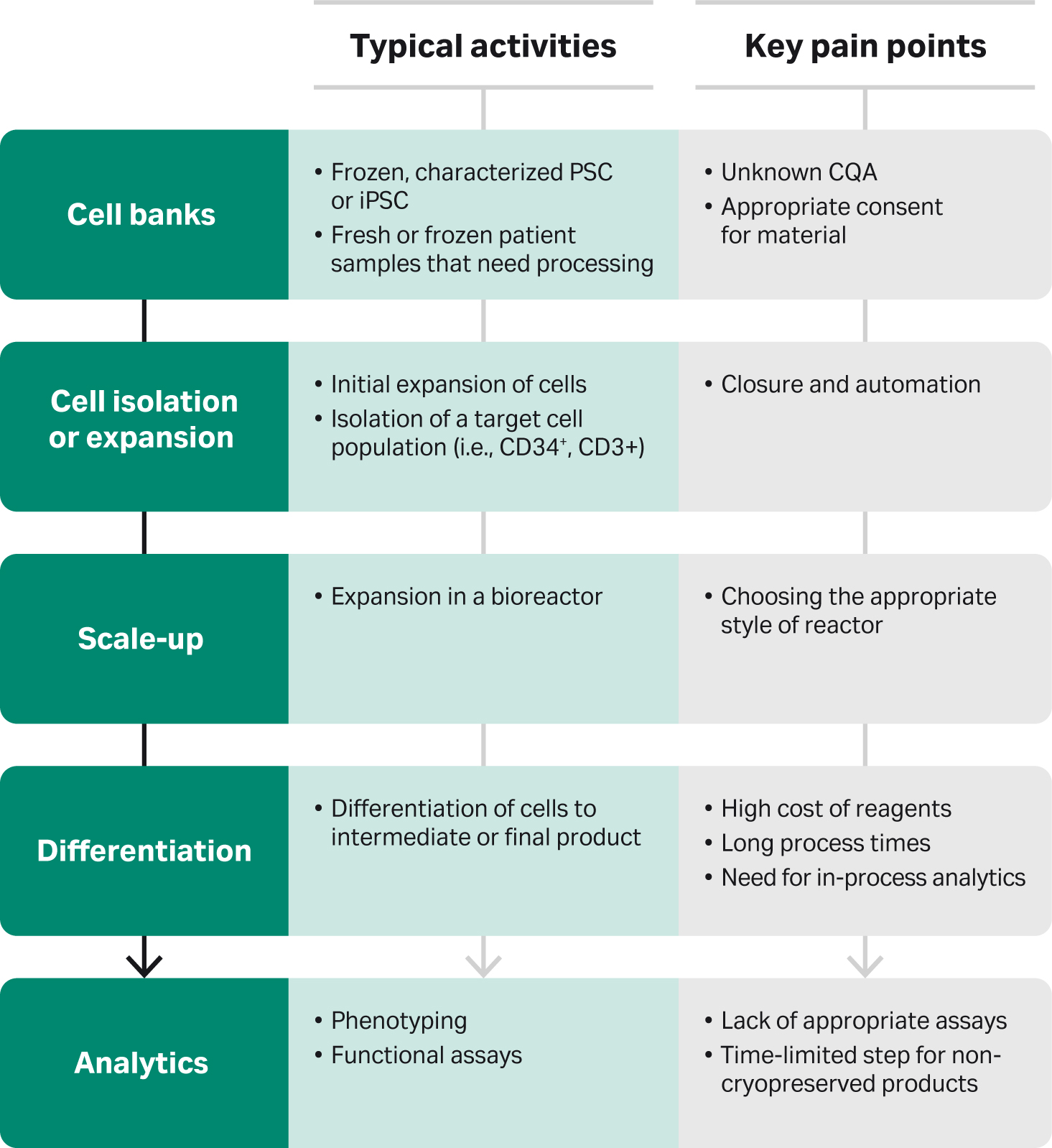
Upstream PD starts with a cell source. In the case of pluripotent stem cells (PSC) or induced pluripotent stem (iPS) cells, the source is often a frozen, characterized working cell bank. On the other hand, an autologous therapy may start with fresh or frozen patient samples. Here, you may be dealing with everything from appropriate consent for the material to working with some unknown critical quality attributes (CQA). You may have a list of things you're looking for in the starting material, or you might not know what you need or how to measure it.
For iPS derived therapies, you need to scale up your starting material and then differentiate to your final product. Reagent cost is high, processing times are long, and appropriate analytics that measure the unique phenotype with functional assays are lacking. Also, you must look at some time-limited steps if you're delivering fresh rather than frozen products. As an industry, we need to deliver live cell therapies to patients, but do we have time to properly analyze them? And what are our potency assays?
You can reduce variability in cell culture by using master cell banks. To reduce variability in the master and working cell banks themselves, you could do various levels of testing. That might be identity, purity, or even genetic stability.
Best practice: Maintain extremely high standards even in the early process steps. Plan ahead for large enough banks to meet regulator needs for testing.
For allogeneic therapies, we rely on the creation of these very large working cell banks. But, for autologous therapies, the cell source is a unique patient sample. Manufacturing is very difficult when you don't know what kind of patient sample is coming in, how it has been stored, etc.
Best practice: Mimic some sample compositions and run your process using these to act as a mimic database for handling different patient samples.
Best practice: Once you have your working cell bank for an allogeneic therapy, focus on cell isolation or initial expansion. Ideally, you want to automate and close this step.
For instance, in the field of pluripotent stem cells and iPS derived therapies, that's often just thawing a frozen vial of cells and growing them out to a certain point in static flasks. This is tedious, time consuming, and open. We can take learnings from unit operations in the immunotherapy field and automate and close this step as early as possible.
Best practice: Closed processing systems will not only minimize operators’ hands-on tasks, which could introduce product-to-product variability or contamination, but also improve manufacturing efficiency. Layering on advanced digital technologies will add flexibility, efficiency, and confidence.
Also, consider how you're going to take this into a good manufacturing practices (GMP) environment, either in-house or at a contract development and manufacturing organization (CDMO). That might include introducing some cold steps or hold times between unit operations to make timing a bit more reasonable in the GMP suites. Starting from when you first get samples in, what things can you build into your process so it won’t go to GMP with a 24-hour workflow?
A major challenge for cell-based therapies is scale-up, that is, producing enough cells to meet the preclinical or clinical dose requirements. With T cell therapies you're trying to create enough material to directly treat patients. For iPS therapies you're trying to create enough material for a differentiation protocol. A lot of our iPS differentiation protocols don’t have a great deal of expansion. Sometimes that differentiation comes at the expense of expansion.
If you need at least a billion cardiac cells to treat a patient, you’ll need to scale up the number of pluripotent stem cells to get there. Perhaps you’ll have to combat inefficiency by creating tens of billions just to get a billion cardiac cells for a dose. The number of cells differs wildly between therapies. In contrast to cardiac therapies, an iPS-derived therapy might only require tens of thousands of cells, which is easily doable with hyperstacks or adherent culture. So, it's important to look at as much clinical data as possible to get that dosage appropriate. Also, make sure that you have the data to determine those dosing needs. Because of this variety of scale, there are a lot of equipment options available.
Best practice: Choose a platform that has some scale-down and scale-up options, to keep the flexibility in PD work and have the best translation into production. It’s not always possible but try for that as much as you can.
Also, think about using a platform that can connect and integrate with your accessory systems, so you can close and automate steps from feeding to harvest as early as possible. Although harvest is downstream, getting your downstream and upstream people to talk to each other is critical, because the downstream staff may ultimately have a decision on the platform.
As we’re learning from working with different cell therapies, the cell type can really dictate the platform needed. We can work through a couple of projects where we're looking at taking adherent cultures and moving them to full suspension. But some projects might require interaction with a cell matrix. You may need to consider some different platforms, and the cells will drive that need.
If you have created some really high density cell banks, you might be able to seed stirred-tank bioreactors directly and skip the first three unit operations. Although there's so much historical data on how to do it with mAb production, we're just getting there now with stem cells. It took a lot of work to reach the efficiency and efficacy of a Chinese hamster ovary (CHO) cell vial process. Certainly, we’ll need a lot of process development to achieve that with stem cells, but we're on our way.
As is true for bioprocessing, it’s important to think about availability of raw materials, supply chain, cost of goods, single supplier, etc. Also, consider producing growth factors and small molecules in-house and moving to xeno-free and animal component-free to support manufacturable clinical processes.
Key learnings for pluripotent stem cells
We're often taking processes that work very well in a small scale. But they're expensive, lengthy, and sometimes do not translate from static to suspension.
Best practice: Have a well-defined quality target product profile (QTPP) supported by evidence. Introduce CQAs early.
When you're scaling up, perhaps working in ten liters, you need to know as soon as possible if that run is deviating from the norm. You do not want to find out on day 21. We think that always goes hand in hand with developing analytical tools. We want to move as much as we can to in-process analytics and predictive analytics and look at focusing on functional and potency assays.
Best practice: Develop analytical tests in the PD lab so they can be qualified for manufacturing. Make sure they’re robust and quantitative. It’s important to have analytical tools that match up with what you’re doing for PD.
Of all the lessons we learned, one of the most painful was realizing we didn't have sufficient analytics at different key time points. So, that was something we really needed to work on and continue to work on. We think we're doing better at looking at the entire manufacturing process and then stepping back to upstream and seeing how we can create the best workflow possible with upstream and downstream together.
When developing specialized processes in cell culture, it’s important to think about how they will scale up. For instance, heat shocking a 10 L bioreactor is not as easy as moving a static flask from one incubator to the other. So, these are the operations you need to think about early. They may even affect what platform you use going forward.
Best practice: Think about manufacturing early, because downstream steps can influence upstream choices.
Summary
For PSC and iPS the most challenging upstream step is differentiation of cells to get to that product. Translating a process to suspension required that we sometimes had to start again from the beginning. The biology of cells receiving cues in a bioreactor are quite different from adding media on top of static culture.
Think about manufacturing scale and work backwards to move the biology around to make something reasonable, instead of tackling the biology and then stumbling to figure out the manufacturing. We're learning that we must work with those two in tandem. So, the scale of expansion, while challenging, is achievable.
For the PSC derived therapies we have a backbone. We can figure out a lot of the process parameters to get that. And we can define that well enough or learn how to tweak that slightly to create different starting materials. So, we figure out the back end and then work on getting the differentiations specific for each cell type. Creating ten billion PSCs was a huge challenge. But that's possible now.
View the event video for more tips and details on two case studies.
About Fast Trak Centre for Advanced Therapeutic Cell Technologies (CATCT)
This work was performed at the Fast Trak Centre for Advanced Therapeutic Cell Technologies (CATCT) in Toronto, Canada. This center was conceived in January, 2016 as a joint collaboration between Cytiva, CCRM, and the government of Canada. The center was tasked with developing the next generation of solutions for effective manufacturing of cell and gene therapy products to make these treatments more accessible to patients. In 2020 the center has grown to include more than 100 associates with expertise in process development and optimization, manufacturing, and many other specialties. Learn more about Fast Trak services for cell and gene therapy.